No items found.
Free Webinar · May 7 · How to Get (and Keep) More Patients as a Practitioner →
Save Your SpotTable of Contents

Experience Better Practice Management Today!
Starting at $28.05/month
No Credit Card Required
Experience Better Practice Management Today!
Starting at $30/month
No Credit Card Required
Physiotherapists often start by writing notes just to get through the day. You see, whoever books in, switches between cases, and tries to stay on time. Charting becomes something you rush and promise to clean up later.
Then one day, you open a chart before a follow-up and realize you are not fully clear on what changed or why you chose a certain plan.
Effective SOAP notes fix that. In this article, I’ll cover:
Let’s break it down in a practical way you can use right away.
SOAP notes are not just a record of what happened. They are the thread that connects one visit to the next.
When they’re done well, they make your next decision easier. They stop you from repeating the same questions. They help you catch patterns you might miss when you’re busy. They let another provider pick up the case without guessing.
They also matter when someone else reads them, like an insurer, an auditor, or a regulator. In those moments, your note is not “for you.” It is proof of what you assessed, what you concluded, and why your plan made sense.
And on a normal day, clear notes save time in a very practical way. You do not have to re-learn the case every visit.
Bonus read: 9 AI SOAP Notes Software for Physical Therapists
A good SOAP note is not a long SOAP note. In physiotherapy, effectiveness comes down to clarity. Your note should make sense next week, not just right after the session. It should also make sense to another clinician who has never seen the patient before.
Here’s what that looks like in practice:
A simple check helps. If another physio read your note, could they explain what changed, what you think is happening, and what you plan to do next? If yes, your SOAP note is doing its job.
Strong SOAP notes are built step by step. Each section has a clear role, and when you respect that, your notes become easier to write, follow, and defend.
Let’s go section by section.
Over the last decade, the best SOAP notes I’ve seen in physio clinics all have the same feel. They’re not “perfect,” just easy to follow. You can tell what brought the patient in, what you found, what you think it means, and what you did next.
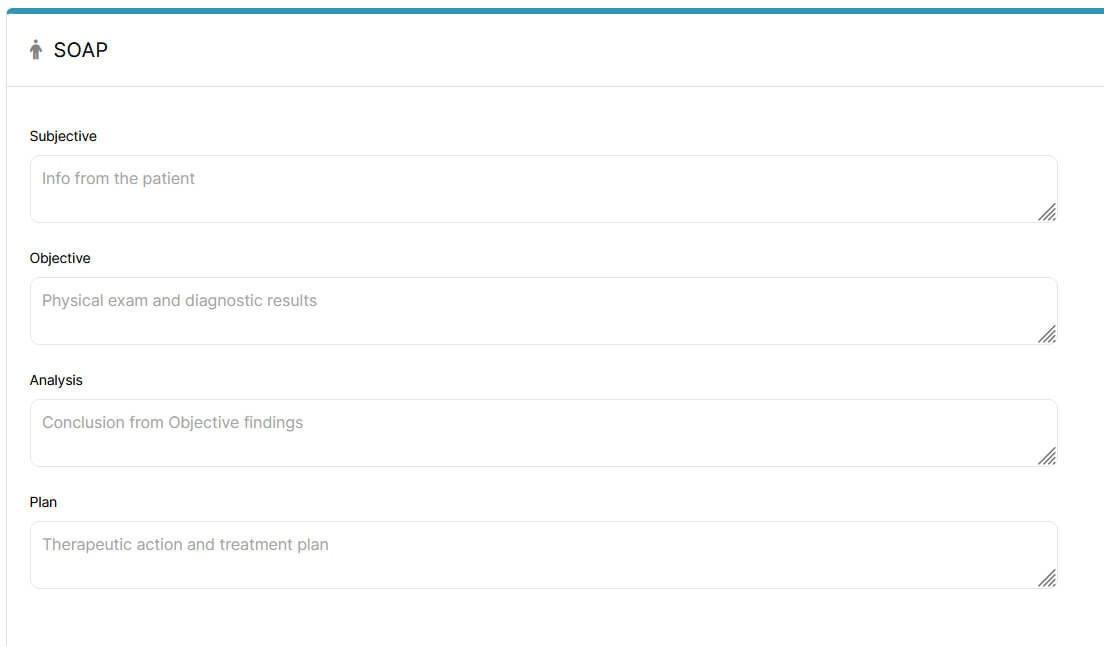
The Subjective section is where you capture what the patient reports. It should answer one core question: “Why did this patient seek care today, in their own words?”
In practice, Subjective is where a lot of notes get messy. Either the history gets copied repeatedly, or the update is so brief that it doesn’t actually help you on your next visit.
I’d suggest you aim for something simple: a concise update that includes the patient’s symptoms, their experience with the problem, and any context that changes the clinical picture, such as new concerns or functional impact.
Here’s the structure that keeps it clear without turning it into a transcript:
Example: Patient reports ongoing right shoulder pain for the past three weeks.
Example: Pain described as a dull ache with intermittent sharp discomfort, rated 6/10, worse with overhead activity and improved with rest.
Example: Patient reports difficulty sleeping on the affected side and reduced tolerance for lifting at work.
Example: Symptoms began after increasing workout frequency. No prior history of shoulder injury reported.
Example: Patient’s goal is to return to regular workouts without pain.
One more thing that matters: don’t diagnose in Subjective. If it’s an interpretation, it belongs in Assessment.
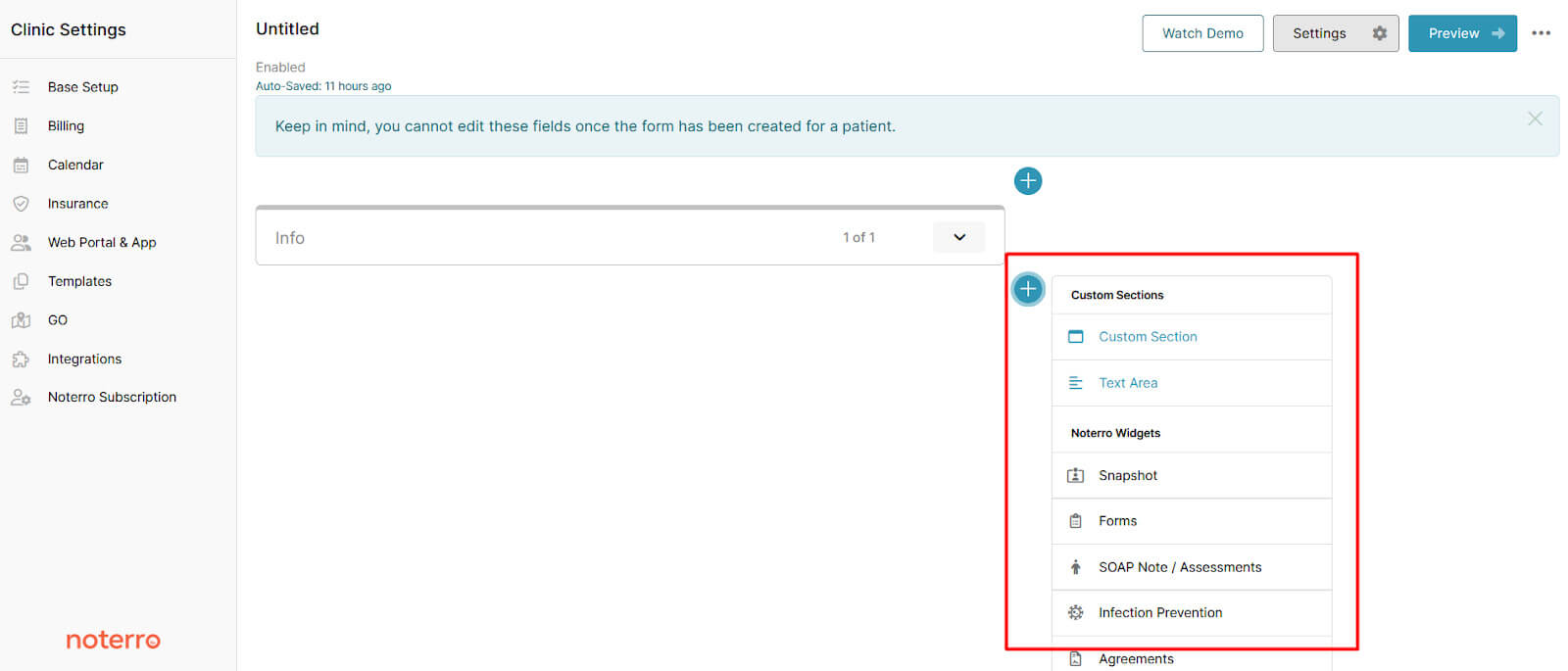
If you want this to stay consistent across visits, it helps to build a structure you can repeat. With custom SOAP note templates from Noterro, you can set up your Subjective section the way you like to think through a case. If you always move from chief complaint to symptom detail to functional impact, your template can reflect that. You’re not rebuilding your format each visit.
Predictive charting and shorthand snippets further cut down repetitive typing by helping you insert common phrasing and adjust it to the current visit, instead of copying from an old note.
The Objective section is where you document what you can observe, measure, or test. It should answer one core question: “What did I observe or assess during this visit?”
The Objective section should stay neutral and focused on observable facts. This is where you document what you saw, measured, and tested, without adding interpretation. Clear, factual entries here give your Assessment a solid foundation.
A well-written Objective section usually follows a simple, consistent flow:
Two simple rules help keep your Objective section clean and defensible. If the information came from the patient, it belongs in the Subjective section. So instead of writing, “Patient reports pain with movement,” document what you observed, such as “Pain observed during active shoulder abduction.”
And if you find yourself interpreting the findings, pause and move that reasoning to Assessment. Rather than writing, “Findings indicate rotator cuff pathology,” record the observable results like this: “Pain reproduced with resisted abduction and positive Hawkins-Kennedy test.” This keeps the Objective factual and lets the Assessment section do its job.
The Assessment section is where your note becomes defensible. It documents your clinical impression based on:
And it answers one core question: “What do these findings mean clinically?”
This is where many notes fall apart, usually in one of two ways: either the Assessment repeats the Objective, or it jumps to a conclusion without showing why.
A strong Assessment has a simple structure:
When these elements are in place, your Assessment section reads like clear clinical reasoning. Just as important, though, is knowing what weakens this section.
Noterro’s physiotherapy management software can support this kind of continuity by linking SOAP sections in a single note, making it easy to reference past visits, and keeping charting tied to the correct appointment.
Related read: 10 Best Physical Therapy Practice Management Software in 2026
The Plan section is where you document:
It answers one core question: “What care is being delivered, and what happens next?”
A clear Plan makes it obvious what happened today and what you’re doing next. That matters for continuity and for reviews. Here’s what to include with examples:
When that structure is in place, your Plan reads clearly and supports continuity. Just as important is knowing what weakens it.
Plans change over time, and you shouldn’t have to rewrite everything to keep them current. In Noterro, easy plan updates and appointment-linked notes make it easier to manage treatment plans.
I see these in solo practices and small clinics all the time. None of these mistakes is catastrophic. But over time, they weaken your documentation and make reviews harder than they need to be.
Here are the big ones to watch for.
When you avoid these patterns, your SOAP notes become clearer, more defensible, and easier to work with day-to-day.
You might also like to read: Chiropractic vs. Physical Therapy Scope: What Clinics Should Know
Audits and insurance reviews usually care less about how long your note is and more about whether it makes sense.
They look for:
SOAP structure helps because it forces alignment. If the Subjective section says one thing and the Plan goes in a different direction, it raises questions.
From a documentation standpoint, consistency and access also matter during reviews. In Noterro, notes are date-stamped automatically, templates can stay consistent across practitioners, and records are securely stored and accessible when needed.

When you can pull up organized, time-linked notes without digging through files, responding to a review becomes much more straightforward.
Over the years, I’ve seen that the physios who feel less burdened by paperwork aren’t writing longer but clearer ones.
When your SOAP notes are structured and easy to follow, you don’t waste time trying to remember what changed or why you chose a plan. You open the chart, and it makes sense. That carries into smoother follow-ups, cleaner handovers, and far less stress during reviews.
I don’t believe documentation should stretch your day or spill into your evenings. It should support your thinking, not drain it.
If you want a system that makes that easier, take a look at how Noterro’s SOAP notes software handles custom SOAP templates, predictive charting, and appointment-linked notes in real clinics.
Tags
Nick Gabriele, Director, Noterro, has been leading the company to greater heights since May 2012. With his vision and 10+ years of expertise, Noterro has become a leading practice management software that offers users an innovative platform for storing notes, tracking appointments, and managing their practice.
Noterro was born out of the need to create a more efficient way to manage paper charts at Ontario College of Health and Technology, which Nick owned.
For nine years, he has performed Independent Medical Evaluations, which allowed him to sharpen his skills in assessing and providing solutions to various health-related issues. With a strong background in rehabilitation settings, including Chiropractic, Physiotherapy, and Massage Therapy, Nick has also garnered a wealth of experience in his field.
Furthermore, Nick has a knack for passion and proficiency in education that has also led him to work in private education for over 20 years. This invaluable experience has enabled him to develop a deeper understanding of how to deliver top-notch training and support to individuals and organizations alike.
In addition to his professional achievements, Nick is an active speaker and has participated in several webinars and podcasts on topics related to electronic record-keeping and practice management. He also has written a plethora of leadership articles on tech topics, including "Charting in the electronic age," "How to Leverage Practice Management Software." His work has been featured in top industry publications, such as Hamilton News. Nick’s insights also have been cited in notable Podcasts like Business Blueprint and Practiciology.


.webp)
No credit card required. Available 1-on-1 support.
.webp)
No credit card required. Available 1-on-1 support.
.webp)
.webp)




.webp)